


 Sign Out
Sign Out

* (See PHARMACOLOGY as follows.)
Pharmacology: COZAAR XQ: The results of two bioequivalence studies in healthy subjects demonstrated that the COZAAR XQ (amlodipine/losartan) 5/50 mg and 5/100 mg combination tablets are bioequivalent to co-administration of corresponding doses of amlodipine camsylate and losartan potassium (COZAAR) as individual tablets with the exception of Cmax for losartan in the 5/50 mg study. This difference was not considered clinically significant.
Amlodipine: The bioequivalence of amlodipine besylate and amlodipine camsylate was evaluated in a randomized, single blind, crossover comparative study conducted in 18 healthy subjects. Groups of 9 subjects received a single 5 mg dose of amlodipine besylate or amlodipine camsylate. Treatments were then crossed over after a 4 week washout period. All 18 subjects received both treatments and completed the study.
Pharmacokinetic parameters including tmax, Cmax, AUC, and half-life were similar following single 5 mg doses of amlodipine besylate and amlodipine camsylate with no statistically significant differences observed between treatment groups. In particular the 90% confidence intervals for Cmax and AUC(0-144) for the test drug/comparator ratios were 0.891 - 1.118 and 0.955 - 1.248 respectively and within the acceptance interval of 80-125% for bioequivalence. The results obtained in this study demonstrated that amlodipine camsylate 5 mg tablets were bioequivalent to amlodipine besylate 5 mg tablets.
Mechanism of Action: COZAAR XQ: COZAAR XQ combines two agents with complementary mechanisms of action to improve blood pressure control in hypertensive patients: losartan potassium, an angiotensin II receptor blocker (ARB), and amlodipine, a calcium channel blocker (CCB). Losartan blocks the vasoconstrictor and aldosterone-secreting effects of angiotensin II by selectively blocking the binding of angiotensin II to the AT1 receptor in many tissues. Amlodipine is a peripheral arterial vasodilator that acts directly on vascular smooth muscle to cause a reduction in peripheral vascular resistance and reduction in blood pressure.
Losartan: Angiotensin II, a potent vasoconstrictor, is the primary active hormone of the renin-angiotensin system, and a major determinant of the pathophysiology of hypertension. Angiotensin II binds to the AT1 receptor found in many tissues (e.g., vascular smooth muscle, adrenal gland, kidneys, and the heart) and elicits several important biological actions, including vasoconstriction and the release of aldosterone. Angiotensin II also stimulates smooth muscle cell proliferation. A second angiotensin II receptor has been identified as the AT2 receptor subtype, but it plays no known role in cardiovascular homeostasis.
Losartan is a potent, synthetic, orally active compound. Based on binding and pharmacological bioassays, it binds selectively to the AT1 receptor. In vitro and in vivo, both losartan and its pharmacologically active carboxylic acid metabolite (E-3174) block all physiologically relevant actions of angiotensin II, regardless of the source or route of synthesis. In contrast to some peptide antagonists of angiotensin II, losartan has no agonist effects.
Losartan binds selectively to the AT1 receptor and does not bind to or block other hormone receptors or ion channels important in cardiovascular regulation. Furthermore, losartan does not inhibit ACE (kininase II), the enzyme that degrades bradykinin. Consequently, effects not directly related to blocking the AT1 receptor, such as the potentiation of bradykinin-mediated effects or the generation of edema (losartan 1.7%, placebo 1.9%), are not associated with losartan.
Amlodipine: Amlodipine is a dihydropyridine calcium antagonist (calcium ion antagonist or slow-channel blocker) that inhibits the transmembrane influx of calcium ions into vascular smooth muscle and cardiac muscle. Experimental data suggest that amlodipine binds to both dihydropyridine and nondihydropyridine binding sites. The contractile processes of cardiac muscle and vascular smooth muscle are dependent upon the movement of extracellular calcium ions into these cells through specific ion channels. Amlodipine inhibits calcium ion influx across cell membranes selectively, with a greater effect on vascular smooth muscle cells than on cardiac muscle cells.
Negative inotropic effects can be detected in vitro but such effects have not been seen in intact animals at therapeutic doses. Serum calcium concentration is not affected by amlodipine. Within the physiologic pH range, amlodipine is an ionized compound (pKa=8.6), and its kinetic interaction with the calcium channel receptor is characterized by a gradual rate of association and dissociation with the receptor binding site, resulting in a gradual onset of effect.
Amlodipine is a peripheral arterial vasodilator that acts directly on vascular smooth muscle to cause a reduction in peripheral vascular resistance and reduction in blood pressure.
Pharmacodynamics: COZAAR XQ: COZAAR XQ has been shown to be effective in lowering blood pressure. Both losartan and amlodipine lower blood pressure by reducing peripheral resistance. Calcium influx blockade and reduction of angiotensin II vasoconstriction are complementary mechanisms.
Losartan: Losartan inhibits systolic and diastolic pressor responses to angiotensin II infusions. At peak, 100 mg of losartan potassium inhibits these responses by approximately 85%; 24 hours after single and multiple-dose administration, inhibition is about 26-39%.
During losartan administration, removal of angiotensin II negative feedback on renin secretion leads to increased plasma renin activity. Increases in plasma renin activity lead to increases in angiotensin II in plasma. During chronic (6 weeks) treatment of hypertensive patients with 100 mg/day losartan, approximately 2-3 fold increases of plasma angiotensin II were observed at time of peak plasma drug concentrations. In some patients, greater increases were observed, particularly during short term (2 weeks) treatment. However, antihypertensive activity and suppression of plasma aldosterone concentration were apparent at 2 and 6 weeks, indicating effective angiotensin II receptor blockade. After discontinuation of losartan, plasma renin activity and angiotensin II levels declined to untreated levels within 3 days.
Since losartan is a specific antagonist of the angiotensin II receptor type AT1, it does not inhibit ACE (kininase II), the enzyme that degrades bradykinin. In a study which compared the effects of 20 mg and 100 mg of losartan potassium and an ACE inhibitor on responses to angiotensin I, angiotensin II and bradykinin, losartan was shown to block responses to angiotensin I and angiotensin II without affecting responses to bradykinin. This finding is consistent with losartan's specific mechanism of action. In contrast, the ACE inhibitor was shown to block responses to angiotensin I and enhance responses to bradykinin without altering the response to angiotensin II, thus providing a pharmacodynamic distinction between losartan and ACE inhibitors.
Plasma concentrations of losartan and its active metabolite and the antihypertensive effect of losartan increase with increasing dose. Since losartan and its active metabolite are both angiotensin II receptor antagonists, they both contribute to the antihypertensive effect.
In a single-dose study in normal males, the administration of 100 mg of losartan potassium, under dietary high- and low-salt conditions, did not alter glomerular filtration rate, effective renal plasma flow or filtration fraction. Losartan had a natriuretic effect which was more pronounced on a low-salt diet and did not appear to be related to inhibition of early proximal reabsorption of sodium. Losartan also caused a transient increase in urinary uric acid excretion.
In nondiabetic hypertensive patients with proteinuria (≥2 g/24 hours) treated for 8 weeks, the administration of losartan potassium 50 mg titrated to 100 mg significantly reduced proteinuria by 42%. Fractional excretion of albumin and IgG also was significantly reduced. In these patients, losartan maintained glomerular filtration rate and reduced filtration fraction.
In postmenopausal hypertensive women treated for 4 weeks, 50 mg of losartan potassium had no effect on renal or systemic prostaglandin levels.
Losartan has no effect on autonomic reflexes and no sustained effect on plasma norepinephrine.
Losartan potassium, administered in doses of up to 150 mg once daily, did not cause clinically important changes in fasting triglycerides, total cholesterol or HDL-cholesterol in patients with hypertension. The same doses of losartan had no effect on fasting glucose levels.
Generally losartan caused a decrease in serum uric acid (usually <0.4 mg/dL) which was persistent in chronic therapy. In controlled clinical trials in hypertensive patients, no patients were discontinued due to increases in serum creatinine or serum potassium.
In a 12-week, parallel-design study in patients with left ventricular failure (New York Heart Association Functional Classes II-IV), most of whom were receiving diuretics and/or digitalis, losartan potassium administered in once-daily doses of 2.5, 10, 25 and 50 mg was compared to placebo. The 25 mg and 50 mg doses produced positive hemodynamic and neurohormonal effects which were maintained for the length of the study. Hemodynamic responses were characterized by an increase in cardiac index and decreases in: pulmonary capillary wedge pressure, systemic vascular resistance, mean systemic arterial pressure and heart rate. The occurrence of hypotension was dose related in these heart failure patients. Neurohormonal results were characterized by a reduction in circulating levels of aldosterone and norepinephrine.
Amlodipine: Hemodynamics: Following administration of therapeutic doses to patients with hypertension, amlodipine produces vasodilation resulting in a reduction of supine and standing blood pressures. These decreases in blood pressure are not accompanied by a significant change in heart rate or plasma catecholamine levels with chronic dosing. Although the acute intravenous administration of amlodipine decreases arterial blood pressure and increases heart rate in hemodynamic studies of patients with chronic stable angina, chronic oral administration of amlodipine in clinical trials did not lead to clinically significant changes in heart rate or blood pressures in normotensive patients with angina.
With chronic once daily oral administration, antihypertensive effectiveness is maintained for at least 24 hours. Plasma concentrations correlate with effect in both young and elderly patients. The magnitude of reduction in blood pressure with amlodipine is also correlated with the height of pretreatment elevation; thus, individuals with moderate hypertension (diastolic pressure 105-114 mmHg) had about a 50% greater response than patients with mild hypertension (diastolic pressure 90-104 mmHg). Normotensive subjects experienced no clinically significant change in blood pressures (+1/-2 mmHg).
In hypertensive patients with normal renal function, therapeutic doses of amlodipine resulted in a decrease in renal vascular resistance and an increase in glomerular filtration rate and effective renal plasma flow without change in filtration fraction or proteinuria.
As with other calcium channel blockers, hemodynamic measurements of cardiac function at rest and during exercise (or pacing) in patients with normal ventricular function treated with amlodipine have generally demonstrated a small increase in cardiac index without significant influence on dP/dt or on left ventricular end diastolic pressure or volume. In hemodynamic studies, amlodipine has not been associated with a negative inotropic effect when administered in the therapeutic dose range to intact animals and man, even when co-administered with beta-blockers to man. Similar findings, however, have been observed in normal or well-compensated patients with heart failure with agents possessing significant negative inotropic effects.
Electrophysiologic Effects: amlodipine does not change sinoatrial nodal function or atrioventricular conduction in intact animals or man. In patients with chronic stable angina, intravenous administration of 10 mg did not significantly alter A-H and H-V conduction and sinus node recovery time after pacing. Similar results were obtained in patients receiving amlodipine and concomitant beta-blockers. In clinical studies in which amlodipine was administered in combination with beta-blockers to patients with either hypertension or angina, no adverse effects on electrocardiographic parameters were observed. In clinical trials with angina patients alone, amlodipine therapy did not alter electrocardiographic intervals or produce higher degrees of AV blocks.
Clinical Studies: The antihypertensive efficacy of COZAAR XQ was demonstrated in 3 controlled studies involving 646 patients with essential hypertension, 325 of whom were treated with COZAAR XQ for 8 weeks. The primary efficacy variable in all studies was change from baseline in sitDBP at endpoint. Secondary variables were change in sitSBP and responder rates. Clinically significant changes in sitDBP at 8 weeks (the primary endpoint) were demonstrated with COZAAR XQ versus monotherapy (losartan or amlodipine) in the studies performed.
In a double-blind, dose-finding study, a total of 320 patients with mild-to-moderate hypertension received treatments of four combinations of amlodipine and losartan (5/50, 5/100, 10/50 and 10/100 mg) or amlodipine alone (5, 10 mg) or losartan alone (50, 100 mg). All doses were initiated at the randomized dose. At week 8, the combination treatments of COZAAR XQ 5/50 and 5/100 were statistically significantly superior to their monotherapy components in reduction of sitDBP and sitSBP. (See Table 1.)
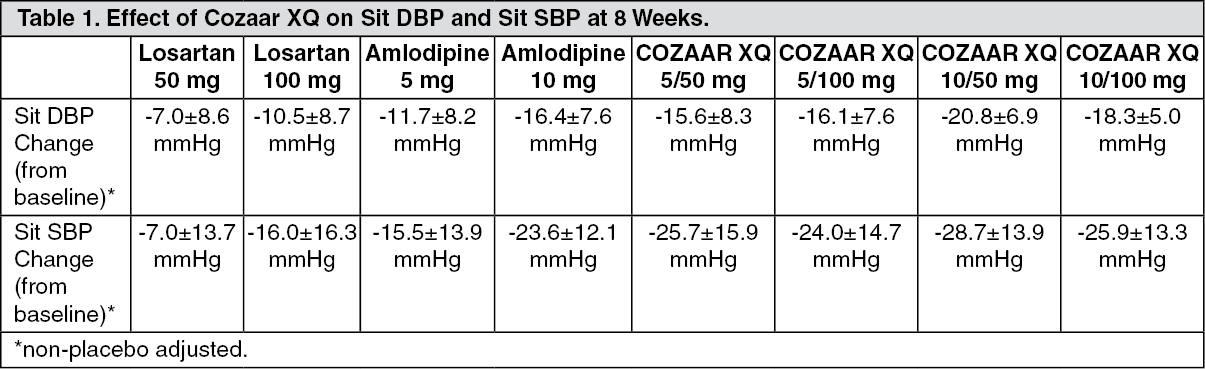 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn a double-blind, active-controlled study, a total of 184 patients with mild to moderate hypertension who were not adequately controlled on amlodipine 5 mg received treatments of either COZAAR XQ 5/50 or amlodipine 10 mg. At week 8, COZAAR XQ 5/50 showed similar incremental BP lowering effects to amlodipine 10 mg. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn a double-blind, active-controlled study, a total of 142 patients with mild to moderate hypertension who were not adequately controlled on losartan 100 mg were switched to COZAAR XQ 5/100 mg or remained on losartan 100 mg. At week 8, COZAAR XQ 5/100 mg showed superior incremental BP lowering effects to losartan 100 mg. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Absorption: Losartan: Following oral administration, losartan is well absorbed and undergoes first-pass metabolism, forming an active carboxylic acid metabolite and other inactive metabolites. The systemic bioavailability of losartan tablets is approximately 33%. Mean peak concentrations of losartan and its active metabolite are reached in 1 hour and in 3-4 hours, respectively. There was no clinically significant effect on the plasma concentration profile of losartan when the drug was administered with a standardized meal.
Amlodipine: After oral administration of therapeutic doses of amlodipine, absorption produces peak plasma concentrations between 6 and 12 hours. Absolute bioavailability has been estimated to be between 64 and 90%. The bioavailability of amlodipine is not altered by the presence of food.
Distribution: Losartan: Both losartan and its active metabolite are ≥99% bound to plasma proteins, primarily albumin. The volume of distribution of losartan is 34 liters. Studies in rats indicate that losartan crosses the blood-brain barrier poorly, if at all.
Amlodipine: Ex vivo studies have shown that approximately 93% of the circulating drug is bound to plasma proteins in hypertensive patients.
Metabolism: Losartan: About 14% of an intravenously- or orally-administered dose of losartan is converted to its active metabolite. Following oral and intravenous administration of 14C-labeled losartan potassium, circulating plasma radioactivity primarily is attributed to losartan and its active metabolite. Minimal conversion of losartan to its active metabolite was seen in about one percent of individuals studied.
In addition to the active metabolite, inactive metabolites are formed, including two major metabolites formed by hydroxylation of the butyl side chain and a minor metabolite, an N-2 tetrazole glucuronide.
Amlodipine: Amlodipine is extensively (about 90%) converted to inactive metabolites via hepatic metabolism with 10% of the parent compound and 60% of the metabolites excreted in the urine.
Elimination: Losartan: Plasma clearance of losartan and its active metabolite is about 600 mL/min and 50 mL/min, respectively. Renal clearance of losartan and its active metabolite is about 74 mL/min and 26 mL/min, respectively. When losartan is administered orally, about 4% of the dose is excreted unchanged in the urine, and about 6% of the dose is excreted in the urine as active metabolite. The pharmacokinetics of losartan and its active metabolite are linear with oral losartan potassium doses up to 200 mg.
Following oral administration, plasma concentrations of losartan and its active metabolite decline polyexponentially with a terminal half-life of about 2 hours and 6-9 hours, respectively. During once daily dosing with 100 mg, neither losartan nor its active metabolite accumulates significantly in plasma.
Both biliary and urinary excretion contribute to the elimination of losartan and its metabolites. Following an oral dose of 14C-labeled losartan in man, about 35% of radioactivity is recovered in the urine and 58% in the feces. Following an intravenous dose of 14C-labeled losartan in man, about 43% of radioactivity is recovered in the urine and 50% in the feces.
Amlodipine: Elimination from the plasma is biphasic with a terminal elimination half-life of about 30-50 hours. Steady-state plasma levels of amlodipine are reached after 7 to 8 days of consecutive daily dosing.
Characteristics in Patients: COZAAR XQ: COZAAR XQ has not been studied in any special populations, due to the well known nature of losartan and amlodipine. Caution is advised for losartan in renal and hepatic impairment, and is contraindicated in breast feeding. No formal studies have been performed in either the elderly or children. For amlodipine caution is advised in hepatic impairment, and amlodipine is contraindicated in unstable cardiovascular disease and pregnancy/lactation.
Losartan: The plasma concentrations of losartan and its active metabolite observed in elderly male hypertensives are not significantly different from those observed in young male hypertensives.
Plasma concentrations of losartan were up to 2-fold higher in female hypertensives as compared to male hypertensives. Concentrations of the active metabolite were not different in males and females. This apparent pharmacokinetic difference is not judged to be of clinical significance.
Following oral administration in patients with mild to moderate alcoholic cirrhosis of the liver, plasma concentrations of losartan and its active metabolite were, respectively, 5-fold and 1.7-fold greater than those seen in young male volunteers.
Plasma concentrations of losartan are not altered in patients with creatinine clearance above 10 mL/min. Compared to patients with normal renal function, the AUC for losartan is approximately 2-fold greater in hemodialysis patients. Plasma concentrations of the active metabolite are not altered in patients with renal impairment or in hemodialysis patients. Neither losartan nor the active metabolite can be removed by hemodialysis.
Amlodipine: The pharmacokinetics of amlodipine are not significantly influenced by renal impairment. Patients with renal failure may therefore receive the usual initial dose.
Elderly patients and patients with hepatic insufficiency have decreased clearance of amlodipine with a resulting increase in AUC of approximately 40-60%, and a lower initial dose may be required. A similar increase in AUC was observed in patients with moderate to severe heart failure.
Sixty-two hypertensive patients aged 6 to 17 years received doses of amlodipine between 1.25 mg and 20 mg. Weight-adjusted clearance and volume of distribution were similar to values in adults.
Animal Toxicology: Acute Toxicity: No single-dose toxicity studies have been conducted with COZAAR XQ.
Losartan: The oral LD50 of losartan potassium in male mice is 2248 mg/kg (6744 mg/m2) (1124 times the maximum recommended human daily dose). Significant lethality was observed in mice and rats after oral administration of 1000 mg/kg (3000 mg/m2) and 2000 mg/kg (11,800 mg/m2) (500 and 1000 times** the maximum recommended daily human dose), respectively.
Amlodipine: In single-dose studies, the approximate lethal oral dose of amlodipine camsylate was 150 mg/kg in rats and 10 mg/kg in dogs.
Chronic Toxicity: COZAAR XQ: Repeated dose toxicity studies of up to 13 weeks with the amlodipine camsylate/losartan potassium combination at a ratio of 1:20 (the highest ratio used in clinical studies) at doses up to 15/300 mg/kg in rats and 2/40 mg/kg in dogs did not result in increase in severity of toxicity or additional toxicities over that observed with the individual substances administered at the highest dose used in the combination. There were no findings that would preclude administration of COZAAR XQ at the therapeutic dosage level.
Losartan: The toxic potential of losartan potassium was evaluated in a series of repeated dose oral toxicity studies of up to three months in monkeys and up to one year in rats and dogs. There were no findings that would preclude administration at the therapeutic dosage level.
** Based on a patient weight of 50 kg.
Carcinogenesis: No carcinogenicity studies have been conducted with COZAAR XQ.
Losartan: Losartan potassium was not carcinogenic when administered at maximum tolerated dosage levels to rats and mice for 105 and 92 weeks, respectively. These maximum tolerated dosage levels provided respective margins of systemic exposure for losartan and its pharmacologically active metabolite over that achieved in humans treated with 50 mg of losartan of approximately 270- and 150-fold in rats and 45- and 27-fold in mice.
Amlodipine: Rats and mice treated with amlodipine maleate in the diet for up to two years, at concentrations calculated to provide daily dosage levels of 0.5, 1.25, and 2.5 amlodipine mg/kg/day, showed no evidence of a carcinogenic effect of the drug. For the mouse, the highest dose was, on a mg/m2 basis, similar to the maximum recommended human dose of 10 mg amlodipine/day. For the rat, the highest dose was, on a mg/m2 basis, about twice the maximum recommended human dose.
Mutagenesis: No mutagenicity studies have been conducted with COZAAR XQ.
Losartan: Losartan potassium was negative in the microbial mutagenesis and V-79 mammalian cell mutagenesis assays. In addition, there was no evidence of direct genotoxicity in the in vitro alkaline elution and in vitro chromosomal aberration assays at concentrations that were approximately 1700 times greater than the maximum plasma level achieved in man at the recommended therapeutic dosage level. Similarly, there was no induction of chromosomal aberrations in bone marrow cells of male or female mice after the administration of toxic oral doses of up to 1500 mg/kg (4500 mg/m2) (750 times the maximum recommended daily human dose). In addition, the active metabolite showed no evidence of genotoxicity in the microbial mutagenesis, in vitro alkaline elution, and in vitro chromosomal aberration assays.
Amlodipine: Mutagenicity studies conducted with amlodipine maleate and amlodipine camsylate revealed no drug related effects at either the gene or chromosome level.
Reproduction: No individual studies have been conducted with COZAAR XQ.
Losartan: Fertility and reproductive performance were not affected in studies with male and female rats given oral doses of losartan potassium up to approximately 150 and 300 mg/kg/day, respectively. These dosages provide respective margins of systemic exposure for losartan and its pharmacologically active metabolite of approximately 150/125-fold in male rats and 300/170-fold in female rats over that achieved in man at the recommended daily dose.
Amlodipine: There was no effect on the fertility of rats treated orally with amlodipine maleate (males for 64 days and females for 14 days prior to mating) at doses up to 10 mg amlodipine/kg/day (8 times the maximum recommended human dose*** of 10 mg/day on a mg/m2 basis).
*** Based on patient weight of 50 kg.
Development: No individual studies have been conducted with COZAAR XQ.
Losartan: Losartan potassium has been shown to produce adverse effects in rat fetuses and neonates. The effects include decreased body weight, mortality and/or renal toxicity. In addition, significant levels of losartan and its active metabolite were shown to be present in rat milk. Based on pharmacokinetic assessments, these findings are attributed to drug exposure in late gestation and during lactation.
Amlodipine: No evidence of teratogenicity or other embryo/fetal toxicity was found when pregnant rats and rabbits were treated orally with amlodipine maleate at doses of up to 10 mg amlodipine/kg/day (respectively, about 10 and 20 times the maximum recommended human dose [MRHD] of 10 mg amlodipine on a mg/m2 basis) during their respective periods of major organogenesis. (Calculations based on a patient weight of 60 kg.) However, litter size was significantly decreased (by about 50%) and the number of intrauterine deaths was significantly increased (about 5-fold) for rats receiving amlodipine maleate at a dose equivalent to 10 mg amlodipine/kg/day for 14 days before mating and throughout mating and gestation. Amlodipine maleate has been shown to prolong both the gestation period and the duration of labor in rats at this dose. There are no adequate and well-controlled studies in pregnant women.